Millions use cannabis, but figures for how many become dependent aren’t reliable
Cannabis has an image of being a relatively harmless drug. But all drugs carry a degree of risk, and cannabis is no exception. One of those risks is dependence, which many people assume is only something that happens to those who use “hard drugs”, such as crack or heroin. In fact, the estimated risk of dependence on cannabis is about one in ten.
This risk may seem relatively low, but given that there are an estimated 200m cannabis users across the globe, the potential number of people who are dependent on the drug is around 20m – roughly, the population of Romania.
It’s worth exploring how this figure of one in ten is constructed. Several studies of cannabis dependence used the criteria (see below) laid out in the American Psychiatric Association’s diagnostic bible, the Diagnostic and Statistical Manual of Mental Disorders (DSM) to determine cannabis dependence.
Examining these criteria highlights just how challenging making this diagnosis is. A reliable way to assess dependence on any drug, including cannabis, is to see what happens when a person stops using it. If they experience physical or psychological withdrawal symptoms, then it is likely they are dependent.
The DSM makes it clear that to qualify for a diagnosis of cannabis dependence, these withdrawal symptoms should not be due to another substance – which is logical but fiendishly difficult to determine in practice. For example, many people mix tobacco with cannabis. Compared with cannabis, the chances of becoming dependent on tobacco are five times greater. So the discomfort people experience when they stop smoking joints could be due to tobacco rather than cannabis. There is considerable overlap in the withdrawalsymptoms of both drugs.
Previous versions of the DSM criteria for substance dependence had a gender bias. One of the questions assessing dependence asked if the person was ever intoxicated while driving a truck. Given that more men drive trucks than women, this raised the dependency criteria threshold for women. Consequently, we have underestimated the number of women who are dependent. Also, cannabis-related offences are greater for men than women. DSM criteria include this issue, again contributing to an underestimate of women.
Psychiatrists decide whether a person qualifies for a diagnosis of cannabis dependence, so, although cannabis is used across the world, most of the data we have about population-level use of cannabis and dependence is drawn from America, Europe and Australia. This significantly limits estimates of cannabis dependence in non-Western countries where there are few psychiatrists.
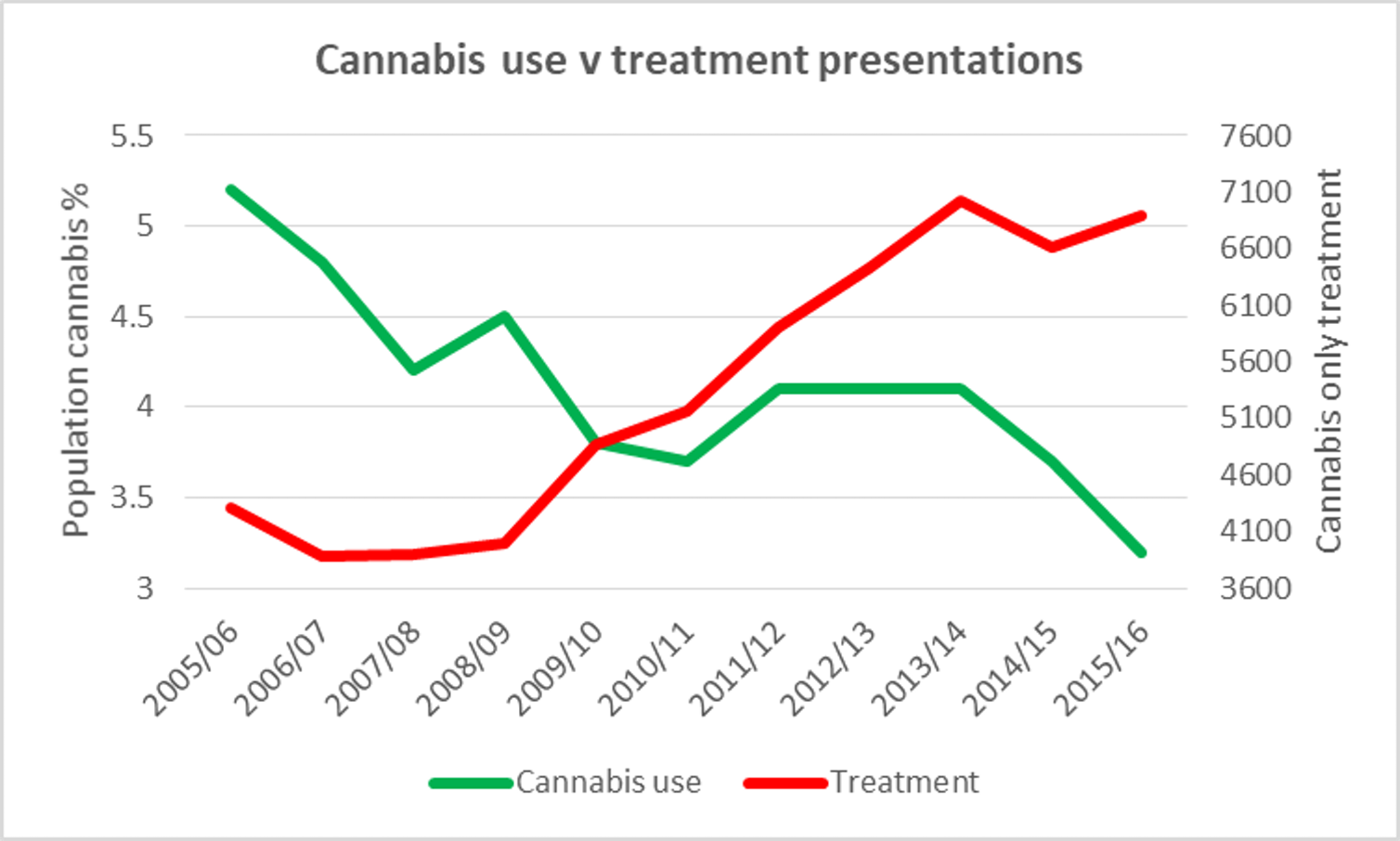
Cannabis use versus treatment. Public Health England & ONS